
Fibrolamellar Carcinoma
Fibrolamellar Carcinoma is a variant of hepatocellular carcinoma
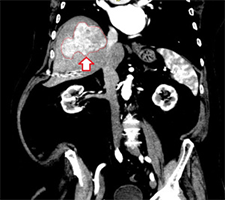
Fibrolamellar HCC is a variant of HCC. It tends to present as a large liver tumor. Complete surgical resection with negative margins is the mainstay of treatment.
Fibrolamellar carcinoma is a type of liver cancer, a variant of hepatocellular carcinoma, which presents unique clinical features and prognosis. The incidence is less than 1 % of all hepatocellular carcinoma and it is mostly occurs in young patients under age of 40 with equal gender ratio. It has no association with chronic liver disease or liver cirrhosis, typically seen in patient with hepatocellular carcinoma. Diagnosis is made with a thin cut contrast CT scan through the liver or MRI scan. Serologic test such as alpha fetoprotein is less helpful. Many patients were referred to a liver surgeon or liver specialist immediacalltoy upon diagnosis. Liver biopsy often done prior to referral. Laboratory workup is consistent with preserved/normal liver function tests. PET scan is sometimes necessary to rule out metastatic lesions somewhere else in the body. Fibrolamellar carcinoma shows increase FDG (glucose) uptake on a PET scan.
Pathologically, fibrolamellar carcinoma is a firm, mostly well-defined but unencapsulated single mass that can range from 5 cm to more than 20 cm in size. It tends to be slow growing and is frequently resectable with a better prognosis than other type of liver cancer. Liver resection with negative resection margins is the goal standard for fibrolamellar carcinoma. When the tumor involves the surrounding organs such as diaphragm, stomach, small and large bowels, then an enbloc organ resection is necessary. The liver cancer treatment starts with a volumetric evaluation of the liver tissue to be resected and liver tissue to be preserved (future liver remnant).
This is done using a highly specialized volumetric CT scan software. Volumetric measurement is critically important for large fibrolamellar carcinomas requiring an extended liver resection removing more than 60-70% of total liver volume. At least 25% of normal future liver remnant has to be preserved in order to avoid postoperative liver failure and death. An experienced liver surgeon can estimate and plan the safest strategy for the extended liver resection, while achieving cure. When the volume of future liver remnant is less than 25%, a preoperative portal vein embolization or portal vein ligation is necessary to induce hypertrophy of the future liver remnant. This is done using interventional radiology techniques, in close collaboration with the liver surgeon. After about 6 week time, a repeat measurement of the future liver remnant volume is conducted to ensure appropriate hypertrophy of the future liver remnant. Successfully resected fibrolamellar carcinoma result in an excellent long-term overall survival and cancer cure. Systemic chemotherapy does not show an effective response to fibrolamellar carcinoma.
Liver transplant surgery is rarely necessary for fibrolamellar carcinoma. Whenever possible, minimally invasive liver surgery should be employed in treating this disease. It is important to see a liver surgeon or liver specialist with extensive experience in liver cancer treatment and large liver tumor resection, often seen with fibrolamellar carcinomas. A multidisciplinary approach is important to achieve best outcomes.
Following a curative liver resection, the patients require follow-up CT scan every 4-6 months for at least 5 years. PET scan is very useful in detecting residual tumors or tumor recurrence after the liver resection. Dr. Iswanto Sucandy has significant experience in managing large liver cancers, including fibrolamellar carcinoma. Dr. Sucandy works collaboratively with interventional radiology experts in Tampa Bay Area to accomplish extended liver resections, which often require preoperative portal vein embolization. In our hepatobiliary center, resection of 70% of the liver volume is undertaken frequently, with great success.

